You checked your blood pressure. Now what?
You sit down with the cuff, wait for the beep, and stare at numbers like 132/84 or 118/76. If you’re wondering what does my blood pressure reading mean, you’re not alone. People search specific fractions after a pharmacy kiosk, a gym health fair, or a home monitor in the kitchen. The number feels personal. It should. Blood pressure is one of the clearest windows into how your heart and blood vessels are working day to day.
Here’s the part that trips people up: a reading is not a diagnosis sitting by itself. It’s a snapshot. Context matters. Were you rushing in from a hot parking lot? Did you just finish coffee? Are you on a new medicine? Your clinician looks at patterns over time, not one spike on a Tuesday.
Still, you deserve plain language about what those two numbers represent and when they deserve a follow-up call. This guide walks through systolic and diastolic pressure, the categories doctors use, and how to tell the difference between “keep an eye on it” and “call today.” If you live in Plano or Collin County, you also know how stress, heat, and long commutes can nudge numbers around. We’ll keep that real-world lens in view without turning every paragraph into local trivia.
The two numbers on the screen
Blood pressure is written as two numbers separated by a slash, like 120/80. The first number is systolic pressure: the force when your heart beats and pushes blood into your arteries. The second is diastolic pressure: the pressure between beats, when the heart rests and fills again.
Think of a garden hose. Systolic is the surge when you turn the tap hard. Diastolic is the steady baseline while the water keeps moving. Both matter. A high top number stresses artery walls over years. A high bottom number can signal resistance in smaller vessels. Doctors weigh both, and they also look at which one is driving a pattern.
Units are millimeters of mercury, written mmHg. You don’t need to memorize that. You do need to know that small shifts can be normal. Standing up quickly, talking during the measurement, or a cuff that’s too small can skew results. That’s why technique and repeat readings help more than obsessing over a single digit.
Public health groups including the American Heart Association describe blood pressure categories using these two numbers together, not in isolation. That combined view is what we’ll use in the next section.
What blood pressure categories actually mean
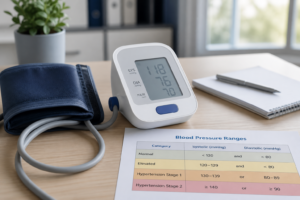
Clinicians group readings into ranges to decide whether lifestyle changes, monitoring, or medication might help. Your personal history still matters. Age, diabetes, kidney disease, and pregnancy can change targets. The table below reflects common adult categories used in U.S. primary care offices today:
| Category | Systolic (top) | Diastolic (bottom) |
| Normal | Less than 120 | Less than 80 |
| Elevated | 120–129 | Less than 80 |
| High blood pressure (stage 1) | 130–139 | 80–89 |
| High blood pressure (stage 2) | 140 or higher | 90 or higher |
| Hypertensive crisis (seek care) | Higher than 180 | Higher than 120 |
A reading lands in the category of whichever number is higher. If your systolic is 128 but your diastolic is 82, you’re in stage 1 because of the bottom number. If you hit 180/90, that’s a different conversation than 132/84, even though both start with a “13.”
Elevated blood pressure is often a warning zone, not a label. Many people pull numbers back with sleep, sodium, movement, and weight changes before medicines enter the picture. Stage 1 and stage 2 usually trigger more structured follow-up: repeat measurements, home logs, labs, and sometimes treatment.
Don’t map every possible fraction to this table. You don’t need a separate paragraph for 114/90 versus 116/88. Look at the range, note the trend, and bring questions to your visit. If you’re unsure where you fall, that’s a fair reason to schedule a blood pressure check rather than scroll through dozens of search results alone.
Why one reading is not the whole story
One reading at a pharmacy or at home is a data point, not a verdict. Blood pressure naturally swings through the day. It’s usually lower during sleep, higher in late morning, and sensitive to pain, caffeine, dehydration, and stress.
That’s why clinicians trust patterns:
- Repeated home readings on different days, taken at the same time, mean more than a single spike.
- Averages over a week beat one dramatic number you got after rushing to an appointment.
- Symptoms paired with numbers (headache, chest pressure, vision changes) change urgency even when the fraction looks “only a little high.”
- Your baseline matters. Someone usually at 108/70 who suddenly hits 145/92 deserves attention faster than someone chronically in the 130s who is already being treated.
If a kiosk reading surprises you, breathe, wait five minutes, and try again with feet flat and the cuff at heart level. Still high on several tries? Write it down and call your primary care office. Still normal? Keep logging occasionally rather than checking hourly. Obsessive checking raises anxiety, and anxiety can raise blood pressure. Not the loop you want.
The CDC notes that nearly half of U.S. adults have high blood pressure, and many don’t know it because it often has no symptoms early on. That doesn’t mean every borderline reading is an emergency. It does mean follow-through beats guesswork.
White coat nerves and home monitors
Some people run higher in clinics than at home. White coat effect is real. You walk in, smell antiseptic, remember the last time you waited forty minutes, and your systolic climbs. Home monitoring helps separate clinic nerves from sustained elevation.
If you buy a home cuff, pick an upper-arm monitor with a validated cuff size. Wrist cuffs are convenient but easier to misuse. Sit quietly for five minutes before the first reading. Feet on the floor, back supported, arm supported at heart level, no talking. Take two readings one minute apart and record the average.
Plano summers add another wrinkle. Dehydration and heat can drop blood volume and make you dizzy when you stand, especially if you’re on diuretics or blood pressure medicines. Hydrate, avoid checking right after a long outdoor walk, and tell your team if standing up feels like the room tilts.
Bring your home log to appointments. A phone note with dates and times is fine. Clinicians would rather see messy real data than a perfect memory of “I think it was high last month.” If home and office numbers disagree often, your doctor may suggest ambulatory monitoring or adjust treatment based on the home pattern.
When a number should get your attention
Not every high reading needs the ER. Many need a conversation and a recheck plan. A few need same-day care. Learning the difference saves panic and prevents delays.
Call your primary care office promptly if:
- Your readings stay at or above 130/80 on multiple home checks and you are not already treated.
- You are on blood pressure medicine and numbers drift above your usual range for several days.
- You have new headaches, vision changes, shortness of breath, chest discomfort, or swelling with higher numbers.
- You are pregnant and see sustained elevation, even if it feels mild.
For a deeper look at timing a visit versus watching and waiting, read when you should go to the doctor for high blood pressure. It walks through symptoms, repeat readings, and what to say when you call.
Some situations need emergency care, not a next-week slot. Severe chest pain, stroke symptoms, trouble breathing, fainting, or a reading at hypertensive crisis levels with symptoms belong in that bucket. Our guide on when high blood pressure is an emergency spells out red flags in plain language. If you’re unsure, nurse triage lines exist to help you sort urgency without guessing.
Primary care in Collin County is built for follow-up: adjusting medicines, reviewing salt and sleep, checking kidney function, and pairing blood pressure work with diabetes or cholesterol when those overlap. One elevated kiosk reading rarely ends the story. It often starts a useful one.
Tracking readings that help your doctor
Good logs are boring on purpose. Same time of day. Same arm. Same posture. Note anything unusual: poor sleep, extra coffee, a new supplement, a stressful work week driving across DNT.
A simple template:
- Date and time
- Reading (systolic/diastolic and pulse if your monitor shows it)
- Context (“felt rushed,” “after morning walk,” “missed BP med last night”)
Track for a week before a visit if your clinician asks for home data. Two weeks is even better when starting or changing medicines. Avoid checking right after exercise, meals, or arguments. Those numbers reflect the moment, not your trend.
At the appointment, ask three practical questions: What range are we aiming for given my history? Which number worries you more in my case? What would make you change my plan before the next visit? Clear targets turn anxiety into action.
If you’ve never had a structured check in a while, pairing a blood pressure conversation with a routine visit is reasonable even when you feel fine. Silent elevation is common. Catching it early keeps treatment simpler and protects kidneys, eyes, and heart over decades, not just this season.
When you’re ready to review your numbers with someone who knows your chart, we’re here. Bring the log, even if it’s scribbled on a receipt from the grocery store cuff. It counts.
Blood pressure reading questions
What is a normal blood pressure reading?
For most adults, normal blood pressure is below 120/80 mmHg. That means systolic under 120 and diastolic under 80. “Normal” doesn’t mean perfect every hour of the day. A single 122/78 after stress isn’t a crisis. Patterns over time tell the story.
Your clinician may set a different target if you have diabetes, kidney disease, prior stroke, or other conditions. Pregnancy uses its own thresholds. Ask what “normal” means for you rather than comparing your log to a neighbor’s.
Which number matters more, top or bottom?
Both matter, and doctors look at whichever is higher when assigning a category. In middle age and beyond, systolic (the top number) often gets more attention because it tends to rise with stiffening arteries. In younger adults, diastolic elevation sometimes shows up first.
Don’t ignore a “only the bottom number is high” pattern. Stage 1 hypertension can be driven by diastolic pressure in the 80s even when systolic looks modest. Share both numbers every time.
Should I worry about one high reading?
One high reading is a reason to repeat the test, not necessarily to panic. Recheck after resting five minutes with proper cuff placement. If the second reading is still high, log it and try again another day at the same time.
Worry more when highs repeat, when you’re already on treatment and numbers jump above your usual range, or when symptoms accompany the elevation. That’s when a phone call beats internet searching.
How often should I check at home?
If your clinician asked for home monitoring, follow their schedule. Common plans include twice daily for a week before a visit, or a few mornings per week when adjusting medicines. Daily checks forever are usually not needed unless you’re in an active titration phase.
Over-checking can fuel anxiety and skew your sense of progress. Consistency beats frequency. Same arm, same posture, same time window when possible.
When should I call my doctor about my numbers?
Call for sustained readings at or above 130/80 if you’re untreated, for repeated highs while on medication, or for any high reading with headache, vision changes, chest pain, shortness of breath, or neurologic symptoms. Pregnant patients should call for persistent elevation even without symptoms.
Call emergency services for stroke signs, severe chest pain, fainting, or crisis-level numbers with symptoms. When unsure, use your clinic’s nurse line. Describing the reading, your symptoms, and your medication list helps them route you correctly.